Injuries in North Korea: Addressing a Looming Crisis
Road crashes, collapsing buildings, work accidents, nuclear weapons, food shortages and human rights dominate the headlines about North Korea. But for ordinary North Koreans trying to make a living, another pressing concern is the exponential increase in the number of injuries in recent years. Due to North Korea’s inadequate trauma care capacity, injuries often result in disability or, even worse, death and impose large economic costs. This is a hidden crisis that the international community should help address.
The Scope of the Problem
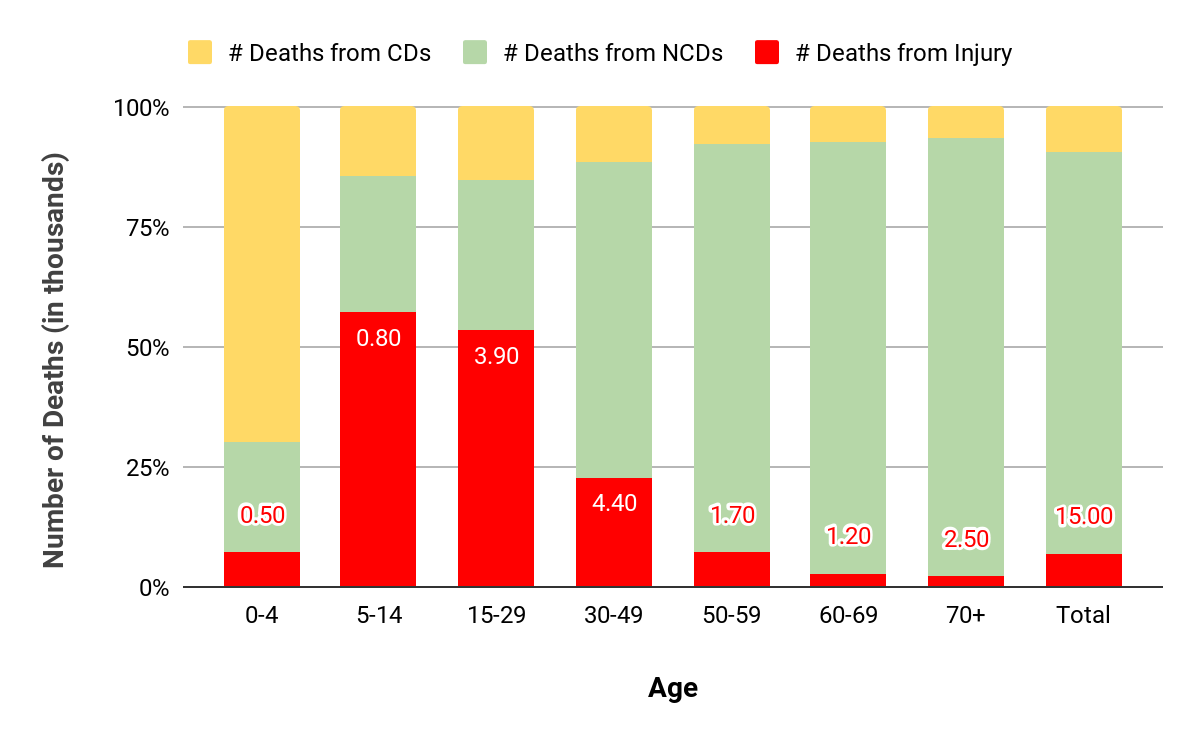
According to the World Health Organization (WHO), injuries are the fourth leading cause of death in North Korea. About 15,600 North Koreans die from injury every year. Furthermore, injuries are by far the biggest killer among the youth and the working-age populations, accounting for more than half of all premature deaths in ages 5 to 29. Road accidents are the most prevalent cause of these fatalities, comprising a third of all injury-related deaths. Falls account for 10.9 percent and mechanical injuries account for 5.1 percent. This suggests work injuries are one of the top causes of death in North Korea. In fact, North Korea’s injury burden is similar to that of other developing countries.
Figure 1. Top ten causes of death in the DPRK
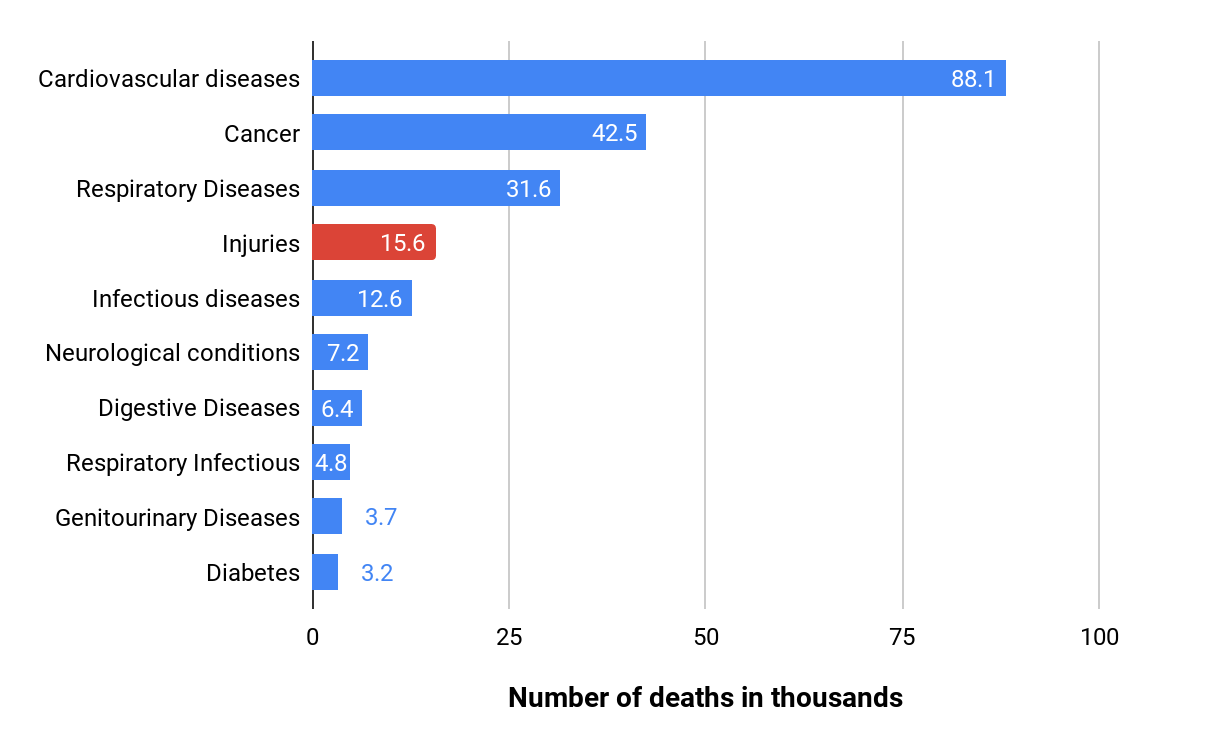
Figure 2. Causes of death in the DPRK by age
North Korea’s health care system and its capacity to deal with the causes and consequences of trauma is inadequate. Based on our survey data, there is room for significant improvement of North Korea’s injury care system: access to hospital care needs to be improved; professional pre-hospital care is essentially nonexistent; ambulance services are unreliable at best; medical facilities, especially outside Pyongyang, often lack the necessary equipment and facilities; and access to drugs in hospitals is minimal and patients frequently have to procure them in local markets (jangmadang). Growing economic activity in North Korea—a construction boom in Pyongyang and elsewhere across the country, increases in road traffic and new multinational industrial and infrastructure projects—will increase the injury burden.
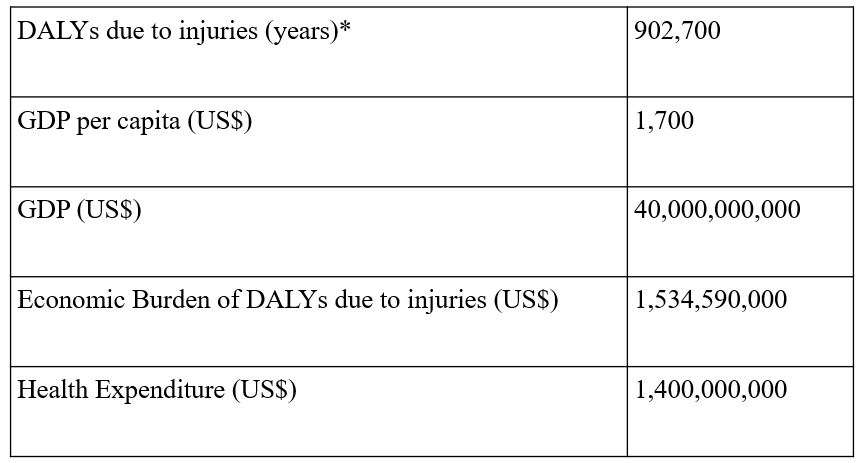
The economic costs of North Korea’s injury crisis are huge. For instance, in 2016 alone, using the WHO’s Disability Adjusted Life Years (DALY) approach (see Table 1), North Korea lost US$1.5 billion as the result of the deaths and disabilities due to injuries. In other words, North Korea lost 110 percent of its annual health spending due to injuries that year. This is a massive macroeconomic loss for any developing country economy, not to mention the societal losses for the injured and their families. Since most of the injured are of working age, they are less productive and can become a “burden” to their communities.
Table 1. Values used to calculate the economic burden of disability-adjusted life years (DALYs)* due to injuries in the DPRK
Implementation Road Map for Building Injury Care Capacity
In a recent report, we and our co-authors analyzed North Korea’s current and expected injury burden and laid out a road map for the international community to partner with the North to scale up its injury care capacity.
Pyongyang voted in favor of the World Health Assembly resolution adopted in 2015 by all WHO members that calls for the “strengthening of emergency and essential surgical care and anesthesia as a component of universal health coverage.” The United States was a co-sponsor of the resolution. In compliance with the mandates of the resolution, the DPRK’s Ministry of Public Health’s (MoPH) most recent 2016-2020 plan for developing the North’s health sector declared its intent to improve the capacity of all first referral level hospitals in the provinces to provide timely emergency and essential surgical care. That is, the health ministry wants to upgrade more than 200 hospitals outside of Pyongyang and improve the skills of its medical personnel.
The WHO and the MoPH have held discussions to launch and implement an operational plan to achieve this goal. Should the plan be initiated, an assessment of North Korea’s needs should be performed on a sample of county hospitals and referral facilities in all ten provinces. The assessment could be carried out by the WHO and/or United Nations Children’s Fund (UNICEF) in collaboration with the MoPH, and would involve consultation with key internal and external stakeholders. Implementation involving the UN agencies would also bring rigorous monitoring and evaluation stipulations that are required from these international organizations.
A similar project by the WHO and UNICEF facilitating the upgrading of approximately 60 county hospitals for improving maternal and child health took place from 2005-2015. The cost of the project was approximately $60 million. By comparison, the cost of national projects to strengthen surgical care have ranged from $400-700 million in countries such as Zambia and Tanzania, respectively. Based on these cases, the cost to scale up North Korea’s injury care capacity would be under $1 billion. In doing so, it would have the added benefits of strengthening North Korea’s capacity to treat other conditions that affect mothers and children, such as emergency obstetrics and congenital conditions, and helping reduce rural-urban disparities by targeting district hospitals outside of Pyongyang.
North Korea, like other developing countries, lacks the domestic resources to fully finance such a program. It is one of the poorest countries in Asia and its economy is shrinking—by 3.5 percent in 2017 according to the Bank of Korea. But Pyongyang should still be asked to contribute to this program to show a commitment to its implementation. This is why we suggest a co-financing model, which is common in developing countries. Indeed, Pyongyang’s work since 2002 with Gavi, the global Vaccine Alliance, as well as its joint project with the Global Fund to fight AIDS, tuberculosis and malaria between 2010 and 2018 follow this model.
Crucially, a program to improve North Korea’s injury care capacity can be implemented even under the current UN Security Council and US sanctions regimes on Pyongyang. Humanitarian assistance, such as medical and health projects, is explicitly excluded from these regimes. Aware of the negative impact that sanctions were having, the UN Security Council has taken a less stringent approach towards exemptions related to the delivery of humanitarian assistance in recent months. Similarly, the US government has also shown a willingness to ease restrictions on the provision of humanitarian assistance from US NGOs. For example, as of this writing, US citizens traveling to North Korea to provide humanitarian assistance are no longer blocked from doing so.
Humanitarian Aid Effectiveness
There is debate regarding whether the international community should deliver aid to North Korea considering the funding priorities of its government. We believe that humanitarian assistance should be separated from this and related considerations, such as North Korea’s nuclear program. Humanitarian aid, including injury care, should be based on need only and not be linked to achieving political objectives. Above all, it is ordinary North Koreans, the youth in particular, who suffer from the country’s weak injury care system.
Similarly, there are questions regarding whether aid actually reaches its ultimate beneficiaries. International organizations and NGOs actually operating in North Korea, however, have settled this debate. As the Office of the Resident Coordinator in the DPRK has made clear, there are robust implementation, coordination and monitoring mechanisms in place. In addition, program implementers have access to aid recipients across all provinces in the country. There is no reason to believe that this would not be the case with a more robust injury care program.
Conclusion
From a purely humanitarian perspective, this program would benefit ordinary North Koreans who have no say on their government’s health care policies and are the most affected by the country’s injury crisis. Cooperation between Pyongyang and Seoul on a multinational initiative to build a comprehensive injury care system in North Korea would be a welcome confidence building measure and demonstrate that greater integration with the international community can bring important economic benefits to the North.
Additionally, from a humanitarian perspective, meeting the increasing burden of injuries in North Korea by scaling up emergency surgical care is an essential public health intervention in preventing deaths and disability, particularly for the young population. Considering that the economic losses due to injuries exceed $1.5 billion annually, there is also a compelling case for investing in the strengthening of the injury care system. The time to invest is now since the burden could increase significantly as the country begins opens up—as was the case in Myanmar.
The geopolitical barriers, as necessary as they are, should not stand in the way of such public health endeavors to improve the lives of ordinary people of North Korea. Practical solutions to the exemption process, logistics and customs barriers, and financial channels are needed to facilitate such massive-scale health projects especially if Pyongyang is able to reach a cooperative approach with multilateral organizations and donors. Multilateral cooperation on health could contribute to regional stability, build confidence and facilitate the integration of North Korea into the international community.